Imagine you're dealing with a severe asthma attack or a sudden, painful flare-up of lupus. Every breath feels like a struggle, and your joints feel like they've been locked in cement. In these moments, Corticosteroids is a class of potent synthetic medications that mimic cortisol, the stress hormone produced by your adrenal glands, to rapidly shut down inflammation. Also known as glucocorticoids, these drugs act like a biological "fire extinguisher," putting out the flames of an overactive immune system almost instantly. But here is the catch: while they are miracles in a crisis, leaving that fire extinguisher running for too long can cause significant damage to your own body.
The Fast Lane to Relief: Why Doctors Use Steroids
When you need a drug to work *now*, corticosteroids are the gold standard. Unlike many other anti-inflammatory medications that take weeks to build up in your system, systemic steroids often start working within 24 to 48 hours. For someone in the middle of a medical crisis, that speed is everything.
The magic lies in their ability to suppress the immune response across the entire body. For example, in cases of peritonsillar abscesses, these medications can reduce the need for surgery by about 27%. If you have severe asthma, they can shave nearly two days off your hospital stay. This rapid efficacy is why they are indispensable for acute flares. However, the way they are delivered changes how they work. You might get a pill (the most common method), an inhaled puffer, a cream, or a direct injection into a joint. While a pill works quickly, a cortisone shot in a knee might take up to seven days to hit full effect, but the relief can last for several months.
Not All Steroids Are Created Equal
You've probably heard of prednisone, but that's just one player in a larger family. Doctors choose different steroids based on how long they need the drug to stay active in your bloodstream. This is known as the biological half-life.
| Category | Example Drug | Biological Half-Life | Typical Use Case |
|---|---|---|---|
| Short-Acting | Hydrocortisone | Under 12 hours | Acute adrenal crisis |
| Intermediate-Acting | Prednisone / Prednisolone | 12-36 hours | Autoimmune flares, Asthma |
| Long-Acting | Dexamethasone | 36-54 hours | Severe edema, Chronic inflammation |
The Hidden Cost of Long-Term Use
If short-term use is like a fire extinguisher, long-term use is like flooding your entire house to put out a small candle. Once you move past the 30-day mark, the risk profile shifts dramatically. Your body begins to pay a price for the systemic suppression of inflammation.
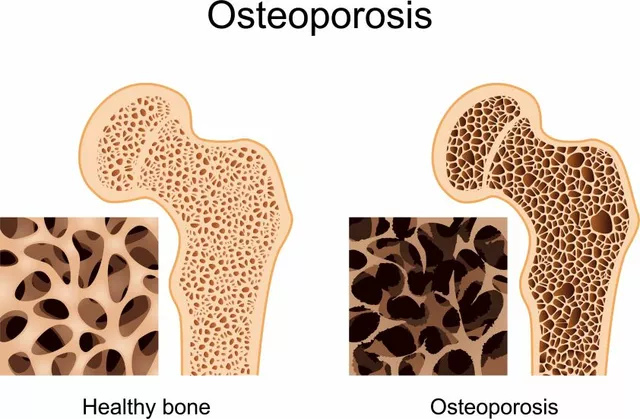
One of the most visible changes is what patients often call "moon face"-a rounding of the face caused by fat redistribution. But the invisible damage is more concerning. Long-term users often experience significant weight gain (averaging over 12 lbs in just two months) and a spike in blood sugar that can lead to steroid-induced diabetes. Your bones also take a hit; bone loss can happen at a rate of 3% to 5% per month during the first year of therapy, which drastically increases your risk of fractures.
Even more serious is the impact on your immune system. While suppressing inflammation is the goal, you also suppress your ability to fight off infections. Short-term courses can increase the risk of sepsis by over 400%. For those using steroids for chronic COPD, there is a notable 15% increase in the risk of pneumonia, which is why doctors try to keep those specific courses under five days.
The Danger of the "Cold Turkey" Stop
One of the biggest mistakes a patient can make is stopping corticosteroids abruptly after a long course. Your adrenal glands are lazy; when you provide synthetic cortisol, they stop producing their own. If you stop the medication suddenly, your body enters a state of adrenal insufficiency, which can be life-threatening.
To prevent this, doctors use a tapering schedule. This means slowly lowering the dose over a week or more to give your adrenal glands time to wake up and start working again. In some cases, if you've been on high doses for a long time, you might even need "stress dosing" of hydrocortisone if you have major surgery, as your body can't produce the necessary cortisol to handle the physical stress of the operation.

Managing the Risks: A Proactive Approach
Since the risks are so high, the goal isn't necessarily to avoid steroids entirely, but to use them with a strict strategy. Modern medical guidelines suggest that for inflammatory arthritis, you should rarely exceed 12 weeks of systemic therapy at the lowest possible dose. If you must be on them longer, a rigorous monitoring protocol is non-negotiable.
- Bone Health: Getting a baseline DEXA scan to monitor bone density and taking supplements like Calcium (1200mg/day) and Vitamin D (800IU/day).
- Blood Sugar: Monthly glucose checks to catch steroid-induced diabetes early.
- Eye Care: Quarterly visits to an ophthalmologist to check for cataracts, which are a known side effect of long-term use.
The goal is to transition from these "bridge" medications to DMARDs (Disease-Modifying Antirheumatic Drugs) or biologics. While DMARDs take much longer to work-sometimes 4 to 12 weeks-they treat the underlying cause of the disease rather than just masking the inflammation, and they don't carry the same metabolic baggage as steroids.
The Future: Smarter Steroids
Medical science is finally moving toward "selective" treatment. In late 2023, the FDA approved fosdagrocorat, a selective glucocorticoid receptor modulator. The idea here is to keep the anti-inflammatory benefits while skipping the metabolic nightmares. Early data shows a 63% lower incidence of high blood sugar compared to traditional prednisone. It's a massive step toward getting the relief without the "moon face" and bone loss.
How quickly do corticosteroids work?
Systemic corticosteroids typically provide relief within 24 to 48 hours. However, localized treatments like cortisone injections into a joint can take up to seven days to reach their full therapeutic effect.
Can I stop taking my steroids immediately if I feel better?
No. If you have been taking corticosteroids for more than 14 days, stopping abruptly can cause adrenal insufficiency because your body has stopped producing natural cortisol. You must follow a tapering schedule managed by your doctor.
What are the most common long-term side effects?
Common long-term risks include weight gain, insomnia, high blood pressure, osteoporosis (bone loss), cataracts, and the development of Type 2 diabetes due to elevated blood sugar levels.
Why are steroids used for asthma but not for a common cold?
Steroids treat inflammation, not viruses. While they are life-saving for asthma (which involves airway inflammation), they provide negligible benefit for uncomplicated upper respiratory infections (colds) and actually increase the risk of secondary infections.
Do all steroids cause weight gain?
While not everyone reacts the same, systemic corticosteroids frequently cause weight gain by increasing appetite and altering how your body distributes fat. Survey data shows that a vast majority of users report weight gain during extended courses.